

From #ThereForME to #ThereWithYou
Doing participatory research with Long Covid patients

Today’s post is from Beth Greenhough and Maaret Jokela-Pansini. Beth Greenhough is Professor of Human Geography at the School of Geography and Environment, University of Oxford, and a Fellow of Keble College. Maaret Jokela-Pansini is a postdoctoral research fellow at the School of Geography and the Environment, University of Oxford, and the Department of Geography, University of Zurich.
Today, Beth and Maaret explore how social science research can help inform the development of a more inclusive NHS for patients with Long Covid and ME.
Why take a social science approach to Long Covid?
We don’t have Long Covid. We didn’t truly understand what having Long Covid could be like until the morning of our first research session working with Long Covid patients.
As social scientists we are interested in learning about people’s experiences of health and illness, and how these are shaped by economic, social and cultural factors such as access to care, gender or living circumstances. The methods we use place a particular emphasis on the importance of patients’ perspectives for making sense of health and illness. We understand health and illness to be embedded within and shaped by everyday life. Academically, Long Covid was interesting to us in part because of its status as the first patient-made disease: a disease which was defined and labelled initially by patients in the absence of a formal clinical definition, diagnostics or treatments.

We knew some statistics about the prevalence of Long Covid, that it impacted some communities more than others, and that it had some things in common with other aspects of health we had worked on in the past, such as community experiences of chronic diseases associated with pollution. What we didn’t know was how profoundly and quickly Long Covid was changing people’s lives, and how all too often their experience was of a government and health service that was not there for them. Patients spoke to us about how they often felt misunderstood, ignored or gaslit by the majority of society. Everyone was talking about the pandemic as if it were in the past, but for the patients we spoke to it remained a dominant factor shaping their day-to-day lives. These kinds of experiences can be profoundly isolating.
Studying patient experiences through body mapping
Our initial project working with Long Covid patients focused on trying to understand women’s experiences of Long Covid. Previous work highlighted that there is a gender dimension to experiences of health and illness, and women’s illnesses are often neglected in research and clinical contexts (think, for example, about recent campaigns to better recognise the impact of menopause or illnesses like endometriosis). We were keen to explore if this might also be the case for Long Covid.
Our plan was to combine interviews with Long Covid patients with a technique called body mapping. Body mapping is an established method in social and health research valued for its ability to capture patient’s lived experiences. In a body mapping session, small groups of participants usually meet in person. The first step is for each participant to create a life-sized outline map of their body. They are then given a list of questions or prompts and asked to respond to these by adding text and images onto their body outline, thereby creating a body map. Further material can be added outside of the body to reflect experiences of the wider environment.
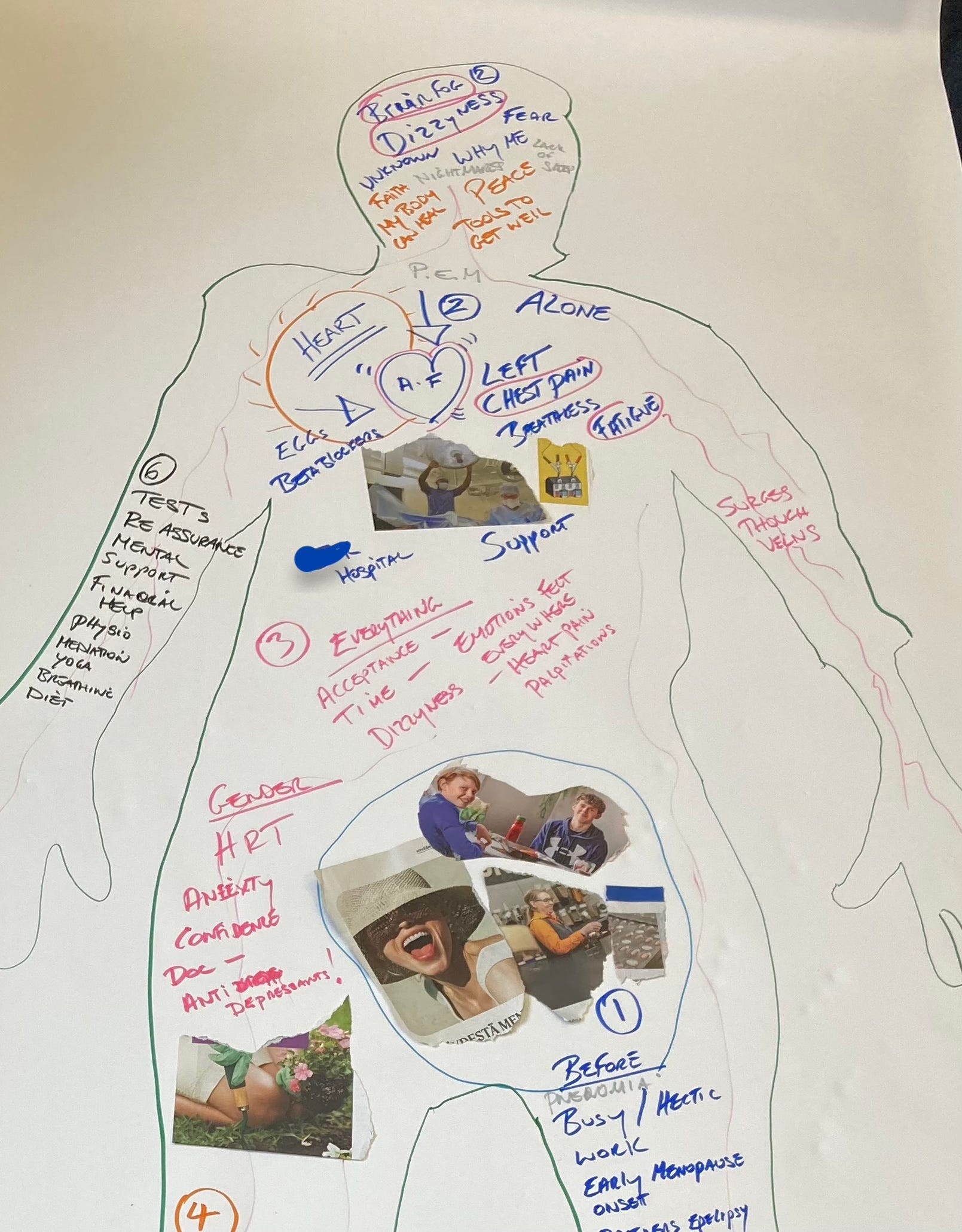
This method is useful as it draws attention to how health is experienced differently across different parts of the body, reflecting how health and illness are embodied experiences. Workshops often finish with a facilitated discussion during which, if they want to, participants share their maps and experiences. Comparing individual body maps between participants can act to highlight moments of shared experience, but also draw attention to the unique and individualised nature of illness, something particularly important for complex chronic conditions such as Long Covid.

Research with Long Covid patients in practice
Despite all our previous work and experience, we were staggered by the stories shared by Long Covid patients at that first workshop. Seeing first-hand the struggle some of our participants had gone through just to get to the room where we were holding the workshop, we were humbled by their determination to participate. We heard heartbreaking stories of lives and futures dramatically changed by chronic illness. We felt inspired by the commitment our participants showed to supporting research and trying to build better futures for themselves and others.
We also saw that body mapping had the potential to be a useful resource for patients who often struggled to find the words to describe their illness to friends, family, and clinicians due to the ongoing impacts of fatigue, brain fog, and the lack of a vocabulary which captured how they were feeling. We were told how our participants found the experience both challenging and rewarding, creating a safe and supportive space to share their stories. It was at this first workshop where we met Oonagh Cousins and Jo Dainow from Long Covid Support and began to see the possibilities for us to work collaboratively with patients to develop research that not only provides insights for social scientists, but can also help meet the needs of Long Covid patients.

Towards collaborative social science research
This initial conversation became the basis for the successful funding application which led to Oonagh becoming an Incoming Engagement Fellow based with us at the School of Geography and the Environment at the University of Oxford. For the past six months we have been working on two projects, which you can read more about on our website. Firstly, we conducted a survey of representatives from across the Long Covid community – patients, carers, researchers, patient support organisations, clinicians – which sought to establish key priorities for future social science research into Long Covid. We plan to publish these as a research agenda later this year with the aim of inspiring and shaping future research projects. Participants’ key concerns included the availability of treatments, the lack of training received by healthcare professionals, barriers to accessing financial support, mental health impacts, and concerns over the risks of reinfection.
Secondly, we developed and piloted an online toolkit based on the body mapping methods for patient facilitators to use in peer support sessions which we will make available through our collaborators at Long Covid Support. A key lesson from these projects is that this kind of collaborative work can inform the development of social science research, building on a growing number of participatory research projects and approaches in health geography and allied disciplines to place the interests, needs and concerns of patients front and centre in its development and design.

Thirdly, Long Covid and ME patients share many core symptoms such as cognitive issues, debilitating fatigue, and post-exertional malaise, and have long struggled to find support from the health care services. Through centring patient experiences, social science research can also serve to evidence the need for developing an NHS which is there for people with Long Covid and ME, drawing attention to the vastly different experiences of those Long Covid and ME patients who felt supported by their clinical teams and those who did not.
We don’t have Long Covid or ME, but by working collaboratively with patients we hope to help inform the development of a more inclusive NHS.
The Long Covid Support Engagement fellowship was supported by the University of Oxford’s Social Sciences Division and funded by the Higher Education Innovation Fund (HEIF). We are also grateful to the charity Long Covid Support for their collaboration and the Swiss National Science Foundation for funding the research project ‘Living in a chronically ill body: Mapping women’s embodied experiences of Long Covid’.
As someone who has had severe ME for 32 years, I’m very pleased that these eminent social scientists have done this report and I hope their conclusion will impress others throughout the whole world of healthcare enough to change attitudes and make it feel safe to have this complex (though not as complex as some researchers would like us to believe!) illness. Alongside funding research, educating HCPs in these illnesses is vital so patients won’t dread Drs and hospitals who don’t understand LC and ME and, frankly, can’t be bothered to try to. At the moment patients feel profoundly unsafe at the mercy of the NHS.
My daughter has just graduated with her BA from Oxford and is about to start her Master's there. Since having covid she has POTS and long covid, the university has been supportive in giving her lift passes for libraries and accommodation without stairs. She has had some tutors who will immediately open windows in tutorials for her. She masks everywhere. She tends to sleep through at least a couple of days a week and had to pace herself very carefully.
I have ME/Fibromyalgia and have done for 30 years. Thank you for your work on this. Did you mask for the workshops/have ventilation/air purifiers?